
The Hidden Language of Healthcare Systems
Every time a patient is admitted to a hospital, something invisible happens behind the scenes. Their demographic details flow from the front desk into the EHR. Lab orders travel to the laboratory system. Radiology gets notified. The billing department gets updated. All of this happens in seconds, without a single phone call or paper form.
The reason this works is HL7. And yet, most healthcare professionals have never heard of it.
For IT directors, EHR administrators, and compliance officers, HL7 is not just a technical term. It is the infrastructure that holds clinical operations together. When it works correctly, care is fast, accurate, and coordinated. When it breaks, the consequences can be serious — from delayed diagnoses to HIPAA violations to revenue loss.
This guide gives you a complete, plain-language understanding of HL7: what it is, how it works, what it powers, and how to implement it securely across your healthcare organization.
HL7 Defined in Plain Terms
HL7 stands for Health Level Seven International. It is a nonprofit standards organization, founded in 1987, whose mission is to create standardized frameworks and messaging protocols for the exchange, integration, sharing, and retrieval of electronic health information.
In practical terms, HL7 is the common language that allows different healthcare software systems to communicate with each other. Without it, an EHR from Epic would not know how to read a lab result sent by a Cerner system. A pharmacy platform would not understand a prescription order from a hospital information system.
Core Definition: HL7 is a set of international standards that define how healthcare data should be structured, formatted, and transmitted between clinical and administrative systems.
The ‘Level Seven’ in the name refers to the seventh layer of the OSI (Open Systems Interconnection) model, which governs application-level communication. HL7 standards operate at this layer, sitting above network protocols like TCP/IP to ensure that the actual meaning of healthcare data is preserved and understood across systems.
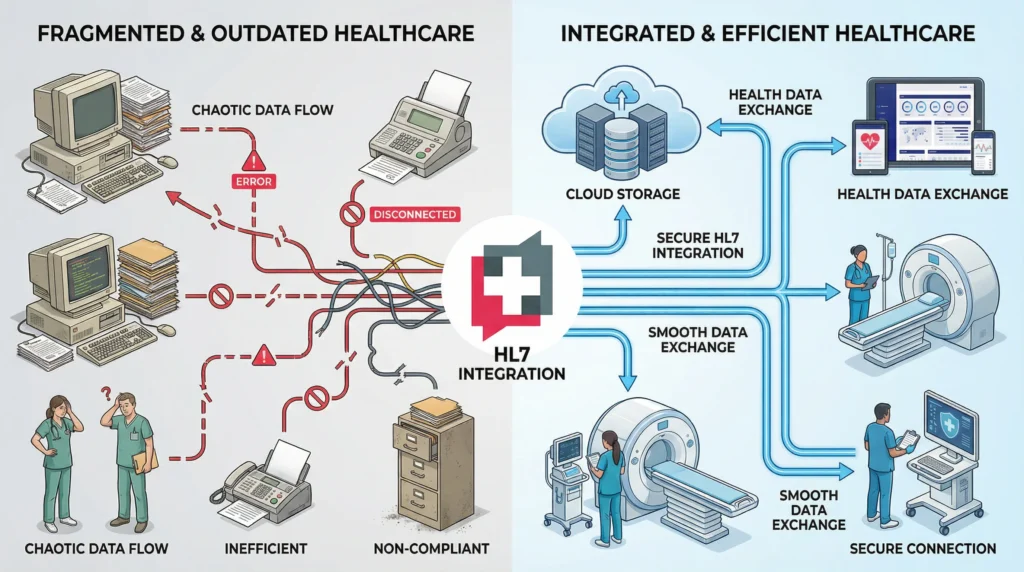
The Problem HL7 Was Built to Solve

Before HL7, every hospital, lab, and vendor built its own proprietary data format. A hospital that used three different vendors for its EHR, radiology, and lab systems effectively had three separate silos of patient data that could not talk to each other without expensive custom interfaces.
This created clinical risk. Physicians made decisions with incomplete information. Labs re-ran tests because results were not visible in the EHR. Billing errors multiplied. Patient care suffered.
HL7 solved this by establishing a common standard. Instead of every vendor building custom interfaces to every other vendor, everyone follows the same messaging rules — reducing integration cost, clinical error, and operational complexity across the entire healthcare ecosystem.
Inside the Architecture of HL7 Data Exchange
Understanding how HL7 works does not require a computer science degree. At its core, HL7 messaging is about structured messages that travel between systems when specific clinical events occur.
Message Structure: Segments, Fields, and Triggers
An HL7 v2 message is a structured text string. It is made up of segments (rows of data), each starting with a three-letter code that identifies its purpose. For example, the MSH segment is the message header and contains routing information, while the PID segment contains patient identification data.
Each segment is divided into fields, separated by pipe characters (|). Each field contains specific data elements such as a patient’s last name, date of birth, or medical record number.
Messages are triggered by clinical events. An ADT^A01 message, for example, is sent whenever a patient is admitted. An ORU^R01 message carries lab results back to the ordering system. These event-driven triggers make HL7 a reactive, real-time communication system.
HL7 Version 2.x — The Backbone of Legacy Healthcare
HL7 v2.x, first released in 1989 and updated through v2.9, remains the most widely deployed healthcare messaging standard in the world. Industry data consistently shows that approximately 95% of US healthcare organizations still use HL7 v2 in some capacity.
Its durability comes from its simplicity. HL7 v2 messages are text-based, relatively easy to implement, and broadly supported by every major EHR, lab, and radiology platform. Most hospitals that have been operating for more than a decade have significant HL7 v2 infrastructure already in place.
However, HL7 v2 has real limitations. It is not natively web-friendly, lacks a formal standard for security, and allows significant local customization that can create interoperability problems between organizations.
HL7 Version 3 and CDA — When XML Entered the Room
HL7 v3 was introduced to address the inconsistencies of v2 by using a formal object-oriented model with XML-based messaging. In theory, this made messages more semantically rich and machine-readable.
In practice, v3 was complex and expensive to implement. Many organizations that adopted it struggled with the steep learning curve. Its adoption remained significantly lower than v2.
Clinical Document Architecture (CDA), a product of the HL7 v3 effort, fared better. CDA became the standard for clinical document exchange — used for discharge summaries, referral letters, and continuity-of-care documents. It was incorporated into Meaningful Use requirements in the US, giving it broad real-world adoption.
HL7 FHIR — The Modern API-Driven Standard
Fast Healthcare Interoperability Resources (FHIR), released by HL7 International in 2014 and reaching a normative release in 2019 with FHIR R4, represents a fundamentally different approach to healthcare data exchange.
Where HL7 v2 sends structured text messages over hospital networks, FHIR uses RESTful APIs — the same architectural style that powers the modern web. Healthcare data is organized into small, modular units called Resources (Patient, Observation, Medication, etc.) that can be accessed, updated, and shared using standard HTTP methods.
This makes FHIR cloud-friendly, mobile-friendly, and dramatically easier to implement for developers. In 2020, both CMS and ONC published rules requiring healthcare organizations to implement FHIR-based APIs to support the 21st Century Cures Act, making FHIR adoption a compliance requirement, not just a best practice.
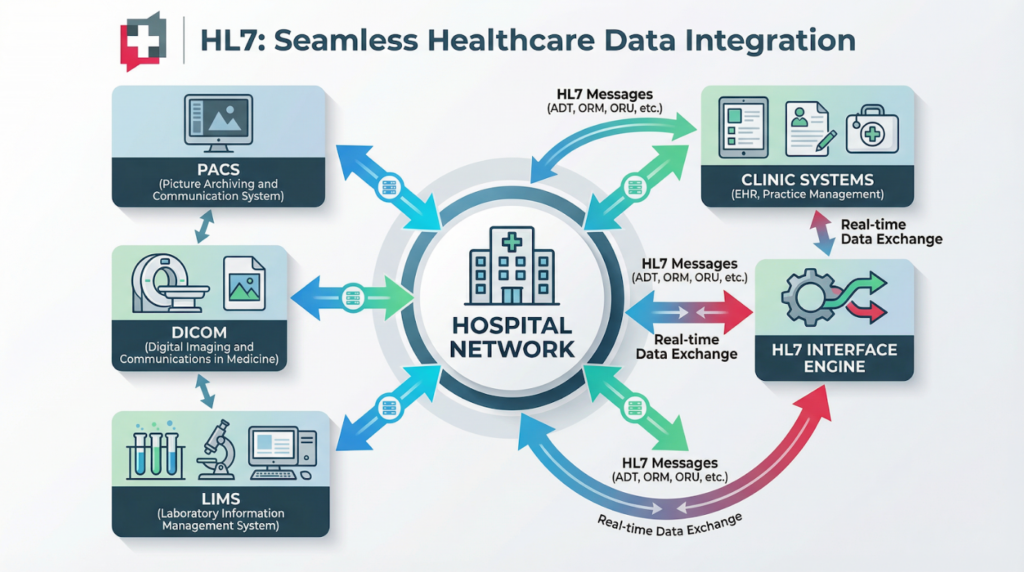
How Hospitals and Clinics Use HL7 Every Day
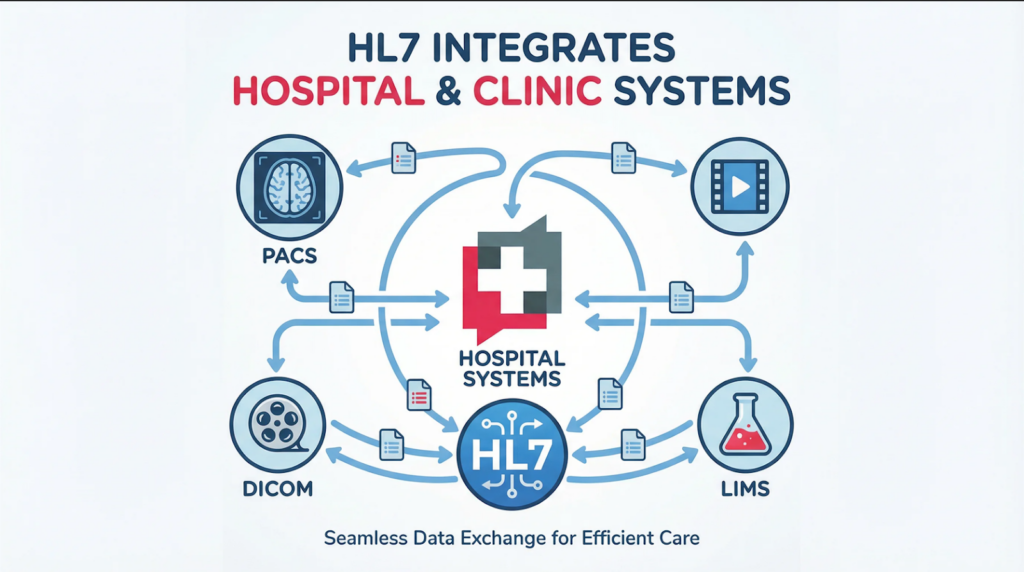
HL7 integration is not an abstract concept. It powers the clinical workflows that healthcare staff rely on from the moment a patient walks through the door.
Admission, Discharge, and Transfer (ADT) Workflows
The ADT workflow is the heartbeat of hospital operations. Every admission, discharge, transfer, and registration event generates an HL7 ADT message. These messages notify every connected system simultaneously — the EHR, billing, the nursing floor system, pharmacy, and the care management platform.
Without HL7 ADT integration, staff at each system would need to manually enter patient information, creating duplication, delays, and the risk of transcription errors. With it, a single registration event at the front desk propagates accurate patient data across the entire organization in real time.
Lab Orders and Results (ORM / ORU Messages)
When a physician orders a blood panel, an HL7 ORM (Order) message travels from the EHR to the laboratory information system (LIS). The LIS processes the order and, when results are ready, sends back an HL7 ORU (Observation Result) message to the EHR.
This automated loop eliminates the phone calls, faxes, and manual result entry that once characterized lab workflows. Results appear directly in the patient’s chart, attached to the ordering provider, complete with critical value flags. Faster results mean faster clinical decisions — and in time-sensitive cases, that difference is measurable in patient outcomes.
Radiology, Pharmacy, and Billing Integration
Radiology systems receive HL7 ORM messages for imaging orders and send back structured reports. Pharmacy platforms receive HL7 RXO (Prescription Order) messages and communicate dispensing confirmations. Billing systems receive charge data through HL7 DFT (Detail Financial Transaction) messages, enabling automated claims generation.
Each of these workflows would be a manual, error-prone process without HL7. Together, they represent the digital nervous system of a modern healthcare organization.
Remote Patient Monitoring and Wearables
In 2025, HL7 FHIR has extended into home care and wearable technology. Devices that monitor blood glucose, heart rate, blood pressure, and oxygen saturation can push readings directly into a patient’s EHR record via FHIR Observation resources. Care teams receive automated alerts when readings fall outside normal parameters — without the patient needing to call the clinic.
This represents one of the most significant expansions of HL7’s real-world impact: moving data exchange from hospital walls into the patient’s daily life.
The Business Case for HL7 Integration
Clinical benefits are compelling. But for healthcare executives and IT leaders making investment decisions, the business case for HL7 integration is equally powerful.
Eliminating Data Silos and Duplicate Testing
Fragmented systems mean fragmented data. When a patient’s imaging results are in one system and their medication history is in another, clinicians cannot see the full picture. Duplicate testing occurs when providers cannot access existing results — a problem that costs the US healthcare system an estimated $8 billion annually.
HL7 integration connects these silos. A unified patient record means fewer duplicate orders, fewer diagnostic errors, and more confident clinical decision-making.
Faster Clinical Decisions, Better Patient Outcomes
A study by HIMSS found that 75% of clinicians using EHR-integrated applications report that easy access to comprehensive patient data helps them prevent medical errors. The speed at which HL7 delivers data is a direct contributor to this outcome.
In emergency settings, every minute of delay in accessing a patient’s allergy information, current medications, or prior diagnoses is a patient safety risk. HL7-integrated systems eliminate this delay.
Revenue Cycle Management and Billing Accuracy
HL7 integration between clinical and billing systems ensures that every chargeable service is captured and coded correctly. Automated DFT messages reduce the gap between care delivery and billing, speeding up claims submission, reducing denials, and improving net revenue.
For large health systems, even a 1-2% improvement in billing capture rate translates to significant revenue — often millions of dollars annually. HL7 integration is not just an IT project; it is a financial performance initiative.
Reducing Medication Errors Through Connected Records
Medication errors are among the most preventable and costly problems in healthcare. Connected HL7 systems give prescribers, pharmacists, and nurses access to the same up-to-date medication records, allergy lists, and clinical alerts simultaneously. Duplicate prescriptions, contraindicated combinations, and missed allergy flags are significantly reduced when all systems speak the same data language.
HL7, HIPAA, and the Compliance Framework You Cannot Ignore
One of the most common misunderstandings among healthcare IT teams is that implementing HL7 automatically ensures HIPAA compliance. It does not. HL7 defines how data is structured and exchanged. HIPAA defines how Protected Health Information (PHI) must be protected. These are separate concerns that must be addressed together.
Why HL7 Alone Does Not Guarantee HIPAA Compliance
HL7 v2 in particular has no built-in security mechanisms. It does not enforce encryption, authentication, or access controls. If you transmit HL7 messages over an unencrypted network, you are moving PHI in a form that is readable to anyone who intercepts it. That is a direct HIPAA violation.
Many legacy HL7 implementations in US hospitals use MLLP (Minimal Lower Layer Protocol) over internal TCP/IP networks — a pattern that made sense in closed hospital networks but is dangerously exposed in hybrid cloud environments and interconnected health systems.
Securing HL7 Pipelines: TLS, VPN, and Access Controls
Properly securing an HL7 environment requires layering security controls on top of the messaging protocol. Best practices include encrypting all HL7 message traffic using TLS 1.2 or higher, deploying VPN tunnels for connections between facilities, implementing role-based access controls on interface engines, and maintaining detailed audit logs of all PHI transmissions.
Every organization transmitting HL7 data with external partners should also have executed Business Associate Agreements (BAAs) in place with all vendors who touch PHI, as required under the HIPAA Privacy and Security Rules.
The 21st Century Cures Act and the Mandate for FHIR
The 21st Century Cures Act, finalized through ONC and CMS rules in March 2020, established new interoperability requirements for healthcare organizations. These rules require certified EHR systems to implement FHIR R4 APIs that allow patients, providers, and payers to access health information — and they prohibit information blocking.
For healthcare IT teams, this means FHIR adoption is no longer optional for systems seeking ONC certification. Organizations still running purely on HL7 v2 need a clear roadmap for integrating FHIR-based APIs alongside their existing infrastructure.
Business Associate Agreements and Audit Readiness
Any vendor who builds, manages, or accesses HL7 interfaces that carry PHI is a Business Associate under HIPAA. Ensuring that your HL7 integration partner has signed a BAA, maintains documented security controls, and can provide evidence of compliance upon audit is a non-negotiable operational requirement.
MediSure Solution structures all HL7 and FHIR integration engagements with HIPAA compliance as a foundational design requirement, not an afterthought.
HL7 v2 vs FHIR: Choosing the Right Standard for Your Systems
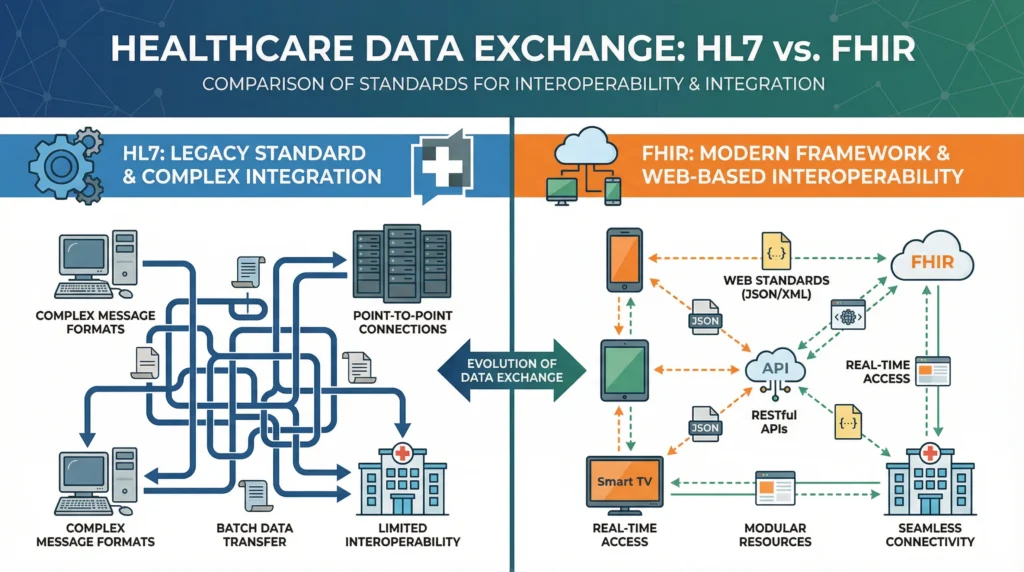
The HL7 versus FHIR debate is one of the most common sources of confusion for healthcare IT teams evaluating integration options. The reality is that these standards are not mutually exclusive — and for most organizations, the answer is both.
When HL7 v2 Still Makes Sense
HL7 v2 is the right choice for maintaining existing internal integrations within a healthcare organization. If your hospital already has hundreds of HL7 v2 interfaces connecting your EHR, lab, pharmacy, radiology, and billing systems, replacing them wholesale with FHIR is neither practical nor necessary.
HL7 v2 also remains the standard for high-volume, low-latency messaging in hospital LAN environments. ADT, ORM, and ORU message flows that process thousands of messages per hour are well-served by mature HL7 v2 infrastructure.
When to Migrate to FHIR
FHIR is the right choice for new integrations, especially those involving external partners, patient-facing applications, mobile health apps, and cloud platforms. It is required for 21st Century Cures Act compliance and is the mandatory standard for CMS and ONC-certified systems.
If you are building a patient portal, launching a telehealth platform, integrating with a payer’s API, or connecting a wearable device program, FHIR R4 is the correct foundation.
The Hybrid Approach Most Healthcare Organizations Use
In practice, virtually every healthcare organization operates a hybrid environment. HL7 v2 handles the internal clinical message flows that have always worked. FHIR APIs handle external connectivity, regulatory compliance, and modern application development.
The most effective integration strategies use interface engines — such as Mirth Connect, Rhapsody, or Cloverleaf — that can process both HL7 v2 messages and FHIR resources, transforming between formats as needed. This preserves the value of existing infrastructure while positioning the organization for the future.
A Practical Roadmap for HL7 Integration
Successful HL7 integration is not just a technical project. It is a clinical, operational, and compliance initiative that requires careful planning, the right tooling, and an experienced implementation partner.
Choosing the Right Interface Engine
An HL7 interface engine is the middleware platform that receives, routes, transforms, and delivers HL7 messages between systems. Leading platforms include Mirth Connect (open-source, widely adopted), Rhapsody (enterprise-grade, used by large health systems), and Cloverleaf (Infor’s enterprise offering). The right choice depends on your organization’s scale, technical capacity, budget, and cloud strategy.
At MediSure Solution, our engineers are certified on multiple interface engine platforms and help organizations select, configure, and manage the right engine for their specific environment.
Planning Your EHR Integration Strategy
Before writing a single line of integration code, healthcare organizations need a clear inventory of their current systems, data flows, and message types. A thorough integration assessment maps every interface, identifies which systems are sending and receiving which message types, and surfaces gaps, redundancies, and security vulnerabilities.
This assessment becomes the foundation for an integration roadmap that prioritizes high-impact, high-risk interfaces first — typically ADT, ORM/ORU, and billing workflows — before addressing lower-volume specialty integrations.
If your organization is planning an EHR migration, system upgrade, or cloud transition, now is the ideal time to modernize your HL7 infrastructure and add FHIR capability. Our EHR integration services at MediSure Solution are designed to manage this complexity from assessment through go-live and ongoing support.
Common Pitfalls and How to Avoid Them
The most common HL7 integration failures stem from four avoidable problems: insufficient testing before go-live, poor error handling that silently drops messages, missing security controls that expose PHI, and inadequate monitoring that leaves interface failures undiscovered for hours or days.
Avoiding these pitfalls requires end-to-end testing with realistic message volumes, automated monitoring with real-time alerts, a documented incident response process, and regular audits of interface performance and security controls.
Partner With a Healthcare IT Team That Speaks HL7 Natively
Healthcare data exchange is too critical to entrust to a generalist IT team. HL7 integration requires a combination of clinical workflow knowledge, interface engine expertise, HIPAA compliance understanding, and project management rigor that most internal IT departments cannot maintain in-house.
MediSure Solution delivers end-to-end HL7 and FHIR integration services for hospitals, clinics, laboratories, and healthcare technology companies. From custom HL7 interface development to FHIR R4 API implementation, our team ensures your clinical systems communicate reliably, securely, and in full compliance with HIPAA and the 21st Century Cures Act.
Ready to connect your healthcare systems? Talk to a MediSure HL7 integration specialist today. We offer a complimentary integration assessment to identify gaps, risks, and the fastest path to interoperability.
Frequently Asked Questions About HL7 and Healthcare Data Exchange
1. What does HL7 stand for and who created it?
HL7 stands for Health Level Seven International. It is a nonprofit, ANSI-accredited standards development organization founded in 1987. Its name reflects its position at the seventh (application) layer of the OSI network model. HL7 International developed and maintains the messaging, document, and API standards used for healthcare data exchange worldwide.
2. What is the difference between HL7 and FHIR?
HL7 is the umbrella organization and its v2.x standard is a text-based messaging protocol used for decades in hospital systems. FHIR (Fast Healthcare Interoperability Resources) is a newer HL7 standard that uses RESTful APIs and JSON/XML resources, designed for modern web and cloud environments. HL7 v2 is ideal for high-volume legacy workflows; FHIR is required for 21st Century Cures Act compliance and modern application development.
3. Is HL7 the same as HIPAA compliance?
No. HL7 defines how data is structured and transmitted. HIPAA defines how Protected Health Information (PHI) must be secured and handled. Using HL7 does not automatically make your data exchange HIPAA-compliant. You must separately implement encryption (TLS), access controls, audit logging, and Business Associate Agreements to meet HIPAA requirements for any HL7 interface that carries PHI.
4. Which EHR systems support HL7 integration?
Virtually all major EHR systems support HL7 integration. Epic offers FHIR-based APIs through its Epic on FHIR program. Cerner (now Oracle Health) supports HL7 v2 and FHIR through its Ignite API platform. Allscripts, athenahealth, NextGen, eClinicalWorks, and MEDITECH all support HL7 v2 messaging and varying degrees of FHIR capability. The depth of integration depends on the specific system version and configuration.
5. How long does HL7 integration take to implement?
A simple point-to-point HL7 interface between two systems can be implemented in two to four weeks. A complex enterprise HL7 integration project covering multiple systems, message types, and FHIR migration may take three to twelve months. Timeline depends on system complexity, data volume, testing requirements, and whether a new interface engine needs to be deployed. A thorough integration assessment before the project begins is the most reliable way to set accurate expectations.
6. What is an HL7 interface engine and do I need one?
An HL7 interface engine (also called a middleware or integration engine) is software that receives, transforms, routes, and delivers HL7 messages between healthcare systems. If you are connecting more than two or three systems, you need an interface engine. Without one, you would need a separate custom integration between every pair of systems. Leading options include Mirth Connect, Rhapsody, and Cloverleaf. MediSure Solution can assess your environment and recommend the right platform.
7. Can HL7 v2 and FHIR work together in the same environment?
Yes, and most healthcare organizations use both simultaneously. Interface engines like Mirth Connect and Rhapsody can receive HL7 v2 messages and transform them into FHIR resources (and vice versa), allowing legacy and modern systems to coexist. This hybrid approach is standard practice and does not require replacing existing HL7 infrastructure.
8. How does HL7 support patient safety?
HL7 directly supports patient safety by ensuring accurate, real-time access to patient data across clinical systems. Connected medication records reduce drug interaction risks. Automated lab result delivery enables faster clinical decisions. ADT message flows ensure care teams have up-to-date patient location and status information. When HL7 interfaces fail, these safety-critical data flows stop — which is why monitoring, error handling, and reliable infrastructure are non-negotiable.
